

Written by MATT FADHIL (edited by ROSIE KIRK)
Did Michelangelo have arthritis? Did Beethoven have syphilis? Did Hitler really only have one testicle?
Whether in a history doco on the SBS or a Buzzfeed article on your Facebook feed, we’ve all come across questions like these at some point or another. What might seem at first glance like the random musings of a history nerd actually find their origins in a well-established field of academic research, a field known as retrospective diagnosis.
Retrospective diagnosis is the practice of coming up with a medical diagnosis for the signs, symptoms or causes of death of long-dead patients. Researchers pick out famous historical figures from decades, centuries or millennia ago, then use modern knowledge and methods to reach a diagnosis that best explains their stories. Though a popular practice in the literature, many commentators have criticised retrospective diagnosis as merely a “fun escape for doctors”, of little historical value. Some have even called for an end to its inclusion in the academic literature. 1 This raises two questions. One: what are the practical and ethical issues that we have to consider when making a diagnosis retrospectively? And two: is there really any role for retrospective diagnosis in medicine today?
Let’s begin with the practical issues, and boy are there issues!
If high school history class taught me anything, it’s that studying history requires you to locate the most relevant evidence on a topic, then to carefully evaluate the evidence for its usefulness and reliability. When it comes to doctors making retrospective diagnoses, these rules often seem to fall by the wayside. Many researchers draw on secondary sources such as non-eyewitness written testimony or artists’ impressions, often dated to centuries after the patient’s lifetime and with clear bias discernible in the composer’s motivations. They’ll then construct a likely diagnosis without properly acknowledging the flimsiness of the evidence. For example, Richard III, the infamous English King, was represented for centuries as a dwarf with a hunched back and a withered hand. Doctors in the modern era were quick to jump on the case, churning out diagnoses ranging from pituitary growth dysfunction to a brachial plexus lesion secondary to difficult breech delivery. In doing so, these doctors never stopped to consider that the descriptions of Richard they were working with were floridly embellished by Tudor-era creatives like Shakespeare, in order to disrepute the defeated Plantagenet dynasty. When Richard’s remains were uncovered in an English car park in 2012, scoliosed but otherwise unremarkable, the extent of these doctors’ cockup was evident for all to see. 2 Clearly, a lack of proper scholarship by doctors looking to retrospectively diagnose detracts big time from the credibility of their conclusions.

Even where the sources used are reliable enough, it can be a real challenge for researchers to translate their medical knowledge across very different biomedical, social and cultural contexts. Perceptions and understandings of disease change greatly over time. What we consider epilepsy today was for the ancient Greeks ‘the sacred disease’, dispensed by the gods. Amongst those affected at the time, many count Socrates, who was known to experience motionless, trance-like states and to hear a “divine voice” or “daimonion” in his head briefly at unexpected moments. When authors scour through biographies of Socrates to support the hypothesis of ‘temporal lobe epilepsy with auditory hallucinations’, it’s not as simple as scanning for convulsions or blank stares or auras. Rather, subtle references to Socrates’ “sacred symptoms” must be spotted, and these distinguished carefully from similar but unrelated passages. 1 The finickiness of this process explains why historians will bend over backwards to analyse primary sources in their original language; that most hobbyist doctors have neither the skills, nor the motivation, to be translating lines from ancient Greek is an unavoidable but considerable limitation.
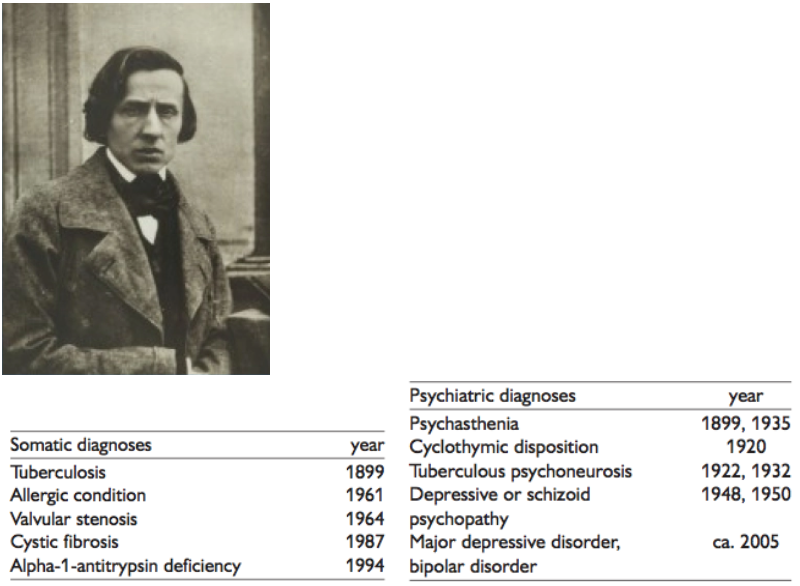
Finally, and most obviously, the patients we’re talking about are dead. Normally, you’d be able to write up a set of differentials based on a thorough history and exam, then run a bunch of investigations on the patient to confirm one differential and exclude the others. Unfortunately, when your patient is already dead, there’s no easy way of talking to, examining or testing them. In other words, it’s all but impossible to verify or falsify any one diagnosis relative to all the others being thrown around. Since medical knowledge is constantly evolving, what’s to stop the diagnoses from becoming more and more elaborate and the list of diagnoses longer and longer? Faced with the unending process of revising and re-revising history, many question why we devote any more time to the question at all. The story of Frederic Chopin is just such a case. Chopin suffered coughs and colds all his life and his mental health was notoriously poor; dozens of articles have been published over the last two centuries attempting to understand why. The explanation for Chopin’s respiratory symptoms has changed from tuberculosis, to cystic fibrosis, to most recently the ultra-specific alpha-1 antitrypsin deficiency. Explanations for his psychiatric symptoms have been just as changeable. 3 Although the evidence for each individual theory is fascinating, we won’t be able to rule in one respiratory diagnosis and exclude all others without the help of genetic testing (a whole separate can of worms, see Lincoln below), and a verdict on Chopin’s psychiatric symptoms is lost to history completely.
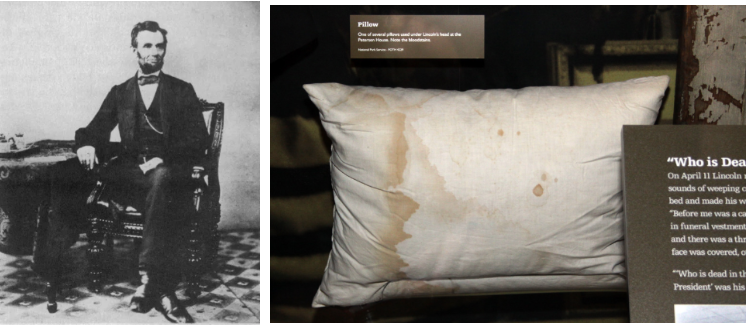
What about the ethics then? On the face of it, retrospective diagnosis seems distinct from the ordinary principles governing clinical medicine: why bother talking about confidentiality when the patient’s dead and all their information accessible online. However, many commentators argue that it’s not that simple. The dead cannot say no, and publishing the good, bad and ugly of a historical figure’s clinical details is a use of medical privilege that doesn’t sit too comfortably with standards of professionalism, especially for recently deceased celebrities. What’s more, for historical figures with living descendants, such investigations can reveal health problems or personal secrets that family members may not want revealed, especially when you introduce genetic testing into the mix. Take Abraham Lincoln. Theories abound about Lincoln’s ill health, with recent publications pointing to a hereditary cancer syndrome called multiple endocrine neoplasia type 2B, accounting for his Marfanoid body shape, abnormal facial features, lifelong depression and the early deaths of his mother and three sons. So, when the Chicago History Museum was approached by scientists in 2009, looking to run DNA tests on artefacts stained with Lincoln’s blood for the purposes of retrospective diagnosis, it turned them all down, citing uncertainty about the wishes of Lincoln’s descendants as well as concerns regarding the effects of experimentation on the fragile artefacts. 4 Other samples have since been studied, with inconclusive results, and in 2019 the verdict on Lincoln’s diagnosis is still out.
Having talked a lot about the problems with retrospective diagnosis, let’s come now to our second question. What, if any, is the role of retrospective diagnosis in medicine today? Well, it’s clear from reviewing the best research in the field that retrospective diagnosis can be much more than just a meaningless hobby for restless diagnosticians. In fact, as an academic practice straddling both history and medicine, retrospective diagnosis offers substantial benefits in both fields.
First and foremost, understanding the diseases afflicting some of history’s biggest names gives us a better insight into why the course of human history progressed the way it did. Knowing that Henry VIII may have been positive for the rare Kell blood group helps us account for the string of failed pregnancies that plagued his first wife, Catherine of Aragon, and therefore Catherine’s failure to produce for Henry a male heir – the consequences of which on English political and religious history need no description. 5 Our capacity to reach such understandings more definitively has been bolstered in recent decades by the use of genetic testing, which has allowed for verification of diagnoses in ways a simple analysis of sources could never hope to achieve. Take Tutankhamun, the young pharaoh, whose life and death have intrigued medical historians ever since the discovery of his tomb in 1922. Diagnoses have abounded to account for the walking canes found buried with the Pharaoh. In 2010, the publication of the results of genetic testing on the remains of Tutankhamun and 15 other royal mummies shed light on these questions and more, confirming definitively that the young Pharaoh had a congenital foot deformity and revealing that he suffered from active malaria, both of which likely contributed to his early death. 6
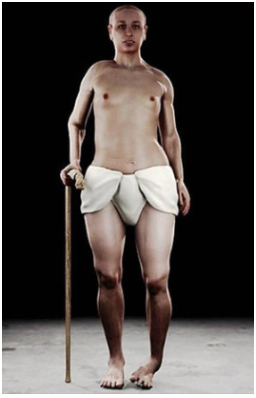
Figure 4. Reconstruction of Pharoah Tutankhamun. Note the deformity of his left foot, for which he likely used a walking stick.
Additionally, in grappling with the practical issues discussed above, we come to understand more clearly the purpose of medical diagnosis and its role in our lives today. We will never know for sure whether Alexander the Great’s death in 323 BC at the age of 32 was due to infection, poisoning or something entirely different. But a publication by Dr Katherine Hall from January this year – in which she outlines a fascinating new theory that Alexander died of Guillain-Barre syndrome and, due to his acute-onset paralysis, was declared dead six days before his actual death 7 – represents as credible a theory as we can hope to achieve. Just like most of the diagnoses we formulate today, Dr Hall’s was a hypothesis constructed to account for all known aspects of the case; was a probabilistic judgement, substantiated by a majority of the critically-examined evidence; and did not have to be incontrovertibly correct in order to be of use (in this case, for re-evaluating the events of Alexander’s last days). Our diagnostic capacities have come a long a way since the days of Alexander, but they’re still far from perfect, as stories of misdiagnosed patients and the catch-all word ‘idiopathic’ would attest to. In attempting to generate diagnoses for a patient dead 2,300 years ago, the exercise of retrospective diagnosis helps reminds us just how limited our diagnostic capacities are, even today. Realising this generates a humility around our approach to diagnosis that’s very much worthwhile.
On balance, I believe there is still a role for retrospective diagnosis in medical literature. Rather than treating the exercise as a game, and in doing so risking the potential ethical harms for little benefit, doctors need to identify from the outset the questions they’re looking to answer in investigating a historical figure. The research must be held to a high standard of scholarship, which might be best achieved by collaborating with medical historians. And the diagnosis reached must be a reasonable one, informative but not overly specific, sensitive to the context of the time.
So the next time you find yourself scrolling through Wikipedia, trying to figure out if Hitler really did only have one testicle, stop and take a breather. It’s worth remembering that what you find is usually unverifiable, often of limited scholarship and most likely needs to be taken with a grain of salt. Once you’ve remembered that though, go right ahead and keep scrolling.
References
1 Muramoto, O. Retrospective diagnosis of a famous historical figure: ontological, epistemic, and ethical considerations. Philosophy, Ethics, and Humanities in Medicine 9, 10, doi:10.1186/1747-5341-9-10 (2014).
2 Lund, M. A. Richard’s back: death, scoliosis and myth making. Medical Humanities 41, 89-94, doi:10.1136/medhum-2014-010647 (2015).
3 Karenberg, A. Retrospective diagnosis: use and abuse in medical historiography. Prague medical report 110, 140-145 (2009).
4 Kean, S. Retrodiagnoses. Investigating the ills of long-dead celebrities. Science 337, 30-31, doi:10.1126/science.337.6090.30 (2012).
5 Whitley, C. B. & Kramer, K. A new explanation for the reproductive woes and midlife decline of Henry VIII. The Historical Journal 53, 827-848, doi:10.1017/S0018246X10000452 (2010).
6 Hawass, Z. et al. Ancestry and Pathology in King Tutankhamun’s Family. JAMA 303, 638-647, doi:10.1001/jama.2010.121 (2010).
7 Hall, K. Did Alexander the Great Die from Guillain-Barré Syndrome? Ancient History Bulletin 32, 106-128 (2019).
Average Rating