

written by MATT FADHIL (edited by KATERINA THEOCHAROUS)
In my article just the other month, I set out to explore the wonderful world of medical eponyms, talking through the fascinating and often unexpected scenarios by which diseases, signs and procedures gain their names.
Taking off the rose-tinted glasses for a moment, though, it doesn’t take long to realise that the world of medical eponyms is not always so wonderful. In fact, the tradition of naming medical terms after historical doctors or patients carries with it a whole string of potential issues, both practical and ethical. Many commentators in recent decades have labelled the use of eponyms impractical, inaccurate and outdated, some even advocating to eliminate eponyms from the medical literature altogether in favour of more standardised terminology 1.
Let’s take a closer look at five problems that can come up with the use of eponyms in medicine and some examples of each.
Problem 01: Uninformative and confusing
One of the most common complaints levelled against medical eponyms is that they’re uninformative, an arbitrarily-chosen name that gives the listener no information about the disease, sign or procedure being discussed. At least when a disease is named in ordinary med-speak, you can break it down into its constituent parts and get an idea what it refers to: translate “bovine spongiform encephalopathy” into “cow-related spongy brain disease” and you’re halfway to mastering neuro. With eponyms, though, we’re unable to extract from the name any hints at all about what it refers to.
Then there’s the confusion of multiple similarly-named diseases to deal with. Take Paget’s disease, named after the renowned 19th century English surgeon Sir James Paget. If you did your MSK Anki deck that morning, you may know to interpret “Paget’s disease” as osteitis deformans, a bone disease characterised by dysfunctional bone remodelling. However, without the qualification “Paget’s disease of the bone”, there’s no way of distinguishing osteitis deformans from Paget’s disease of the breast (a form of intraductal breast cancer) or Paget’s disease of the skin (an intraepithelial cancer commonly involving the anogenital region) 2. And that’s not even to get into Piaget’s theory of cognitive development, probably buried deep in the recesses of your mind from BGD. It’s no wonder that eponyms have been labelled “an impenetrable mystery to the uninitiated”3: for med students and patients alike, eponyms can represent a small but significant barrier to communication and understanding.

Problem 02: Medically inaccurate
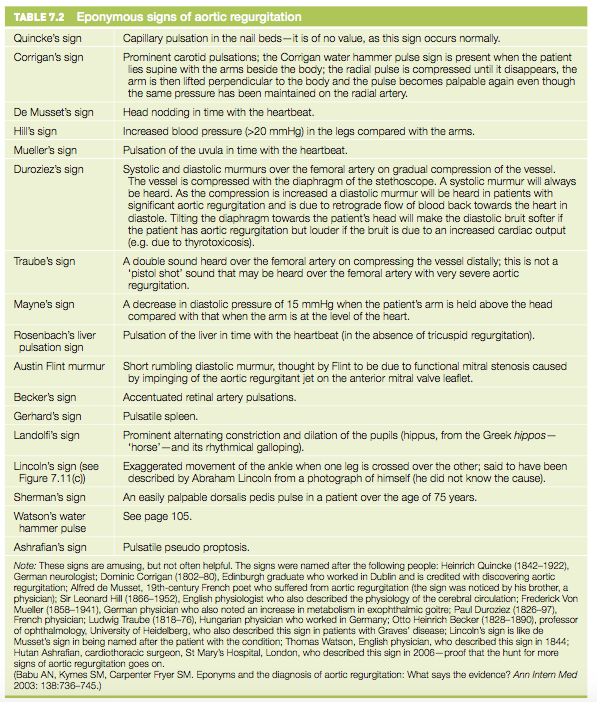
Another problem identified with eponyms is that they’re imprecise, reflecting an archaic understanding of a disease, sign or procedure that doesn’t take into account more recent updates in medical knowledge. After all, if you’re going to get yourself an eponym, the most surefire way would be to make discoveries in an area not-so-well understood – it’s often in the initial stages of a disease’s description, before the full clinical and pathophysiological picture is pieced together, that the names catch on. In many cases, a single poorly-understood medical condition can accumulate a whole litany of eponymous names for its specific features before anyone figures out how to fit them together. Take aortic regurgitation, which over the years has attracted as many as 31 different eponyms for its signs and symptoms 4. There’s actually a whole page of Talley’s just devoted to listing out these eponyms, with a note at the bottom that “these signs are amusing, but not often helpful” 5.
Another result is that very different clinical situations can end up grouped together under the one imprecise name. For decades, Bright’s disease (named after 19th-century British physician Richard Bright) was widely used as an eponym for glomerulonephritis. As our understanding of the different types of glomerulonephritis improved, with their very different causes, pathophysiologies and prognoses, the grouping term “Bright’s disease” became not at all meaningful; its use has since become obsolete 6.
Overall, eponymous names can represent a convenient shorthand for incompletely-understood clinical situations. But once our understanding advances, many argue that this convenience is being purchased at the expense of accuracy and that these eponyms should all go the same way poor Bright’s did.
Problem 03: Historically inaccurate
You may have heard of an Arnold-Chiari malformation, a congenital downward displacement of the cerebellum and medulla through the base of the skull. So who were Arnold and Chiari? Hans Chiari was a 19th-century Austrian pathologist, who, over the course of decades, produced numerous anatomical and pathological descriptions of the congenital malformation that bears his name. Julius Arnold was a German pathologist (with a funky beard) and a contemporary of Chiari’s, who published just one relevant case report. The term “Arnold-Chiari” was coined a decade later by, surprise surprise, two of Arnold’s very own students 7.
And this is just one of many examples of historical inaccuracy in the world of medical eponyms. Whose name sticks and whose doesn’t make the cut is often determined by a whole heap of factors – politics, language, culture, even sheer luck – rather than pure scientific achievement. It’s no coincidence that women are grossly underrepresented in medical eponyms: the contributions of remarkable female doctors and scientists were often dismissed while their male counterparts’ names were immortalised 1. And there are countless cases where the descriptions of the eponymous physician were very obviously not the earliest or best in the literature 3.
Easy solution, you might be thinking, Why leave anyone out? Just chuck all their names on. Well, you idiots are the reason we talk today of Mayer-Rokitansky-Kuster-Hauser Syndrome (congenital agenesis of the vagina and uterus). Taking this idea to its extremes, authors have jokingly proposed acknowledging all those involved in the study of Behçet’s disease (a systemic autoimmune disorder named after 20th-century Turkish dermatologist Hulûsi Behçet) by renaming it Hippocrates-Janin-Neumann-Reis-Bluthe-Gilbert-Planner- Remenovsky-Weve-Shigeta-Pils-Grütz-Carol-Ruys-Samek-Fischer-Walter-Roman-Kumer-Adamantiades-Dascalopoulos-Matras-Whitwell-Nishimura-Blobner-Weekers-Reginster-Knapp-Behçet’s disease 4. I think I’ll stick with Behçet’s, thanks.
Problem 04: Historically inappropriate
Reactive arthritis, formerly known as Reiter’s syndrome, is a form of arthritis triggered by infection elsewhere in the body, most commonly the gut or urogenital tract. Hans Reiter was a German physician who published early descriptions of reactive arthritis in the early 20th century. He was also, unfortunately, a Nazi war criminal. Specifically, Reiter is known to have been complicit in Nazi sterilisation and euthanasia programs and to have committed horrific medical experiments at the Buchenwald concentration camp. The term “Reiter’s syndrome” was proposed in 1942 by Dr Ephraim Engelman, a Jewish rheumatologist, before the extent of Reiter’s complicity was revealed. In an unbelievable twist of fate, it was Dr Engelman himself who issued the callout to rename the term half a century later 8.
Nor is Reiter the only case of a historically tainted eponym: unfortunately, the names of widely-condemned historical figures have infiltrated the catalogue of medical eponyms and are only recently being weeded out. It’s fair to say that having your name taken as an eponym, to be spoken and written day-to-day by doctors and patients, is an honour. Only those who model the ethical and professional responsibilities of being a doctor should be honoured in this way; commemorating those who don’t meet that standard becomes very, very problematic.
A quick final note. The only thing more uncomfortable than a Nazi eponym? A double-barrelled Nazi eponym. That’s right, both Julius Hallevorden and Hugo Spatz, the two men who gave their names to the rare neurodegenerative disorder formerly known as Hallevorden-Spatz syndrome, were fully-fledged members of the Nazi party. Pantothenate kinase-associated neurodegeneration is a bit of a mouthful, but honestly, we’ll take it.

Problem 05: Difficult to use
Last, but very much not least, eponyms can just be difficult. Difficult to say, to write, and to use consistently. There’s the weird and wacky foreign eponyms that you need to be fluent in 17 European languages to pronounce correctly (think Chvostek, Sjogren, Ziehl-Neilsen). There are the dramatic variations in eponyms across countries: sideropenic dysphagia goes by the name Plummer-Vinson syndrome in Australia and the not-so-similar name Waldenstrom-Kjellberg syndrome in Scandinavia6. And there’s the question over whether or not to add the possessive –‘s to an eponym (is it Down syndrome? or Down’s syndrome?), a source of inconsistency that’s inspired countless angry responses to the editor and caused some medical journals to issue flat bans on the use of the possessive 9.
Okay Matt, you’re thinking, I’m convinced. Eponyms are a problem, what’s all the fuss about it, let’s just scrap them. Well, just hold your horses for a second. The core idea of my previous article still holds true: behind every medical eponym is a story, a story about the namesake themselves or about the journey each eponym has taken to end up with that namesake. In this way, eponyms in medicine allow us to stay deeply rooted within medical history, celebrating past discoveries and their discoverers (who, in the vast majority of cases, are NOT Nazis). Even if they just inspire a quick Google search by a patient in the waiting room or a med student after rounds, eponyms spark opportunities to bring the colour and excitement of each individual story to the day-to-day.
There are plenty of other benefits to eponyms too. Sometimes, they’re actually easier to remember than the long convoluted med-speak equivalents: “congenital cyanotic heart disease due to ventricular septal defect, pulmonary stenosis, right ventricular hypertrophy, and aortic dextroposition” is much more taxing on the memory than Tetralogy of Fallot 6. The non-specificity of eponymous names for syndromes, while contributing to imprecision, also allows for their flexibility: provisional labelling is a convenient way for doctors to communicate specific situations to one another and to patients while we improve our knowledge. Last, but definitely not least, eponyms are absolutely everywhere in medicine: you’ll find them in every field in every part of the world, across textbooks, medical school curricula and medical practice. In ENT alone, there are 106 eponymously-named types of forceps 3. Some medical eponyms have become so common and indispensable that we’ve almost forgotten they’re eponyms at all: the Gram stain (G capitalised) is named after 19th-century Danish bacteriologist Hans Christian Gram, who was celebrated in this funky Google logo just the other month.
So what’s the verdict? Should we eradicate eponyms completely? I, for one, believe eponyms are worth keeping. It’s vital that efforts to improve their use continue, like weeding out eponyms that are grossly inaccurate or inappropriate and standardising their grammar and spelling. A little change that has been adopted in the past to much success is to replace the generic noun (“disease”, “syndrome”, etc.) with a more precise term: rather than Albright’s syndrome, why not go with Albright’s hereditary osteodystrophy 3. Regardless, one thing’s for sure: for generations of doctors and students, eponyms are here to stay.
1 Fargen, K. M. & Hoh, B. L. The debate over eponyms. Clinical Anatomy 27, 1137-1140, doi:10.1002/ca.22409 (2014).
2 Buchanan, W. W. Sir James Paget (1814–1894). Rheumatology 42, 1107-1108, doi:10.1093/rheumatology/keg004 (2003).
3 Brunt, R. Medical eponyms revisited. English Today 14, 51-56, doi:10.1017/s0266078400010208 (1998).
4 Woywodt, A. & Matteson, E. Should eponyms be abandoned? Yes. BMJ 335, 424-424, doi:10.1136/bmj.39308.342639.AD (2007).
5 Talley, N. & O’Connor, S. Clinical examination: a systematic guide to physical diagnosis. 7th ed. Elsevier Health Sciences (2014).
6 Whitworth, J. A. Should eponyms be abandoned? No. BMJ 335, 425-425, doi:10.1136/bmj.39308.380567.AD (2007).
7 Solt, I. Chiari malformation eponym- time for historical justice. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 37, 250-251, doi:10.1002/uog.8876 (2011).
8 Panush, R. S., Wallace, D. J., Dorff, R. E. N. & Engleman, E. P. Retraction of the suggestion to use the term “Reiter’s syndrome” sixty-five years later: The legacy of Reiter, a war criminal, should not be eponymic honor but rather condemnation. Arthritis & Rheumatism 56, 693-694, doi:10.1002/art.22374 (2007).
9 Jana, N., Barik, S. & Arora, N. Current use of medical eponyms–a need for global uniformity in scientific publications. BMC Med Res Methodol 9, 18-18, doi:10.1186/1471-2288-9-18 (2009).
Average Rating